
IVF Success Rates by Age. What the Data Shows and What Actually Moves the Needle

Thinking IVF is your only option, or that one cycle is a guarantee?
Here is what the data actually shows and what most people never think to address before starting.
I hated the idea of IVF. I wanted a surprise pregnancy test. I wanted my journey to feel exciting, not like a long, draining process of medications, monitoring, and injections.
If you feel this way, I get it but before you dismiss IVF or rush straight into it, let us take a pause.
Because the question is not really IVF or no IVF. It is when and under what conditions.
Three Women I Know - See If You Recognize Yourself
There is the woman who has been trying naturally for two, three, sometimes four years. She knows IVF exists but she doesn’t want to do it because it feels unnatural. It feels too clinical, too far from the experience she imagined. Maybe the idea of injections and monitoring appointments feels overwhelming. Maybe she is quietly hoping her body will just figure it out if she tries one more thing she read about online. So she keeps going, doing her best, but without a real strategy and without anyone looking at the full picture.
There is the woman who just got diagnosed with infertility, trying for the first or second baby. Her doctor has recommended IVF and she is moving forward. She trusts the process. But she has not changed anything about how she eats, sleeps, or manages stress. Her partner has not either. Nobody has looked at sperm health, thyroid function, inflammation, or anything else that might be quietly working against them. She figures the clinic will handle it. One cycle and she will be pregnant.
And there is the woman who has already done one or two cycles. Maybe three. Each one full of hope and then devastation. She keeps being told to try again but nobody has stopped to ask why it is not working. Her whole-body health has never been part of the conversation. She is exhausted, financially stretched, and starting to wonder if she is missing something.
All three of these women deserve better than what they are getting.
That is the gap WOVA was built to fill.
One Cycle. Here Is What Made the Difference.
One of our clients came to WOVA facing a real challenge: her husband had a male-factor genetic condition, and they needed IVF with embryo testing to rule it out. She was worried about cost, about success rates, about whether one cycle would be enough, and about going through it all without her mom nearby for support.
Instead of defaulting to the most expensive option, we looked at IVF clinics in her home country, closer to family and at a fraction of the cost. While doing an IVF abroad is not the right path for everyone, it was the right path for her family. Then, beyond clinic selection, we spent dedicated time optimizing both her health and her husband's around nutrition, lifestyle, all the factors that actually influence whether IVF works. Even if there is a genetic factor involved, optimizing both partners’ health often leads to better outcomes, healthier pregnancies and healthier children.
She got pregnant on the very first cycle.
Now, you might read that and think: "Well, IVF worked. One cycle, done”.
But here is what most people do not know. For women in the 35 to 40 age group, it takes an average of 2 to 3 IVF cycles to achieve a live birth. Each one costs $25,000 to $35,000, including medications, and carries real physical and emotional weight. First-cycle success is not the norm.
IVF stimulates what is already there. It does not address root causes. The most powerful approach combines personalized whole-body support with IVF.
What The Data Actually Shows About IVF Success Rates
Understanding IVF success rates requires knowing how they are calculated. Clinics typically report live births per embryo transfer, which counts only cycles that made it all the way to having viable embryos to transfer. When you look at live birth rates across all women who started a cycle, including those whose cycles were cancelled before transfer, the numbers look different and knowing both figures helps you plan realistically.
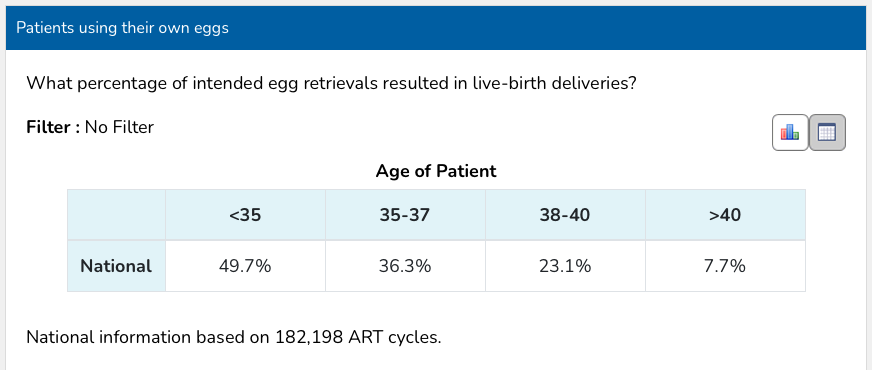
A table showing IVF live birth rates by age group, sourced from CDC/SART 2022. Rates range from 49.7% for women under 35 to 7.7% for women over 40.
The numbers are still meaningful, depending on your age, but they are not a guarantee and knowing the full picture upfront changes how you plan financially, emotionally, and practically.
Here is something worth understanding. If a good, transparent clinic chose to report live birth rates per cycle initiated rather than per transfer, most patients would assume their success rates were lower than competitors even though they were simply being more honest. The same applies to cost. Many clinics quote the procedure fee without medications, which can add another $10,000 to $15,000 on top. Not because they are being deceptive, but because that is the industry standard and quoting the full number would make them look more expensive than clinics quoting selectively.
This is not a criticism of any individual clinic. It is a reflection of how industry-wide reporting norms can make it genuinely difficult for even the most ethical providers to communicate transparently without being penalized for it. Knowing this as a patient means you can ask the right questions rather than comparing numbers that were never designed to be compared.
Is IVF "Natural"? Let Us Talk About That.
“IVF is not natural. I do not want to do it”.
I hear this all the time and I understand it because I used to think the same way. Let’s think about how we live every day for a moment.
Is flying in an airplane natural?
Is scrolling on a smartphone for hours natural?
Is eating ultra-processed foods - your favorite packaged cookies, protein bars, takeout - natural?
Is a hormone-stimulated IUI cycle natural?
We already rely on technology and medical advances in so many areas of our lives. IVF is one of those advances. Millions of babies have been born thanks to IVF, babies who may otherwise never have existed.
So before dismissing it, let us at least look at the full picture. And before rushing into it, let us make sure you are going in prepared.
When Does It Make Sense To Wait On IVF?
Instead of thinking IVF or no IVF, the better question is when and under what conditions.
Consider waiting if:
Whole-body health, yours and your partner's, has not been addressed
Root causes have not been properly investigated
Sleep, stress, inflammation, nutrition, sperm quality, and environmental exposures have not been optimized
You have done 2 or more cycles with no success and nobody has stepped back to ask why
You have not spent at least 3 months intentionally preparing your body before stimulation
IVF may absolutely make sense when:
There are blocked or damaged fallopian tubes where natural conception is near-impossible; IVF bypasses the problem entirely
There is severe male factor infertility - IVF with ICSI can bypass certain sperm limitations
Genetic testing (PGT) is needed for couples with known heritable conditions who need PGT-A to screen embryos
Unexplained infertility after 2+ years of actively trying and after optimizing both partners’ health: spontaneous conception becomes genuinely unlikely, IVF provides meaningful acceleration
Known ovulatory disorders (like certain PCOS presentations where other treatments and whole-body support have failed)
You want to combine IVF with intentional whole-body preconception preparation
A note on diminished ovarian reserve (DOR): Many doctors recommend moving straight to IVF with a DOR diagnosis but it depends. Low ovarian reserve is a marker of egg quantity, not egg quality. Focusing on whole-body health and timing can still make a meaningful difference before or during IVF.
IVF stimulates what is already there. It does not address root causes. The most powerful approach combines personalized whole-body support with IVF.
If you have been trying naturally for 2 to 3 years or more, the conversation shifts. That’s not because natural conception is impossible, but because you deserve answers and because the diagnostic workup that comes with entering an IVF clinic is one of the most valuable and under-appreciated parts of the whole process.
When someone moves forward with IVF, they typically get a level of investigation that rarely happens before that point. A hysteroscopy or sonohysterogram to look inside the uterine cavity identifying polyps, fibroids, a uterine septum, or adhesions that could be blocking implantation. An HSG or saline infusion sonogram to check whether the fallopian tubes are open and the cavity is clear. A full hormonal panel. Sometimes a laparoscopy that finally catches endometriosis that had been quietly working against conception for years.
If a fibroid is found and removed, or a polyp is cleared, or a blocked tube is identified, the pregnancy that follows benefits from that correction, whether it happens via IVF or naturally. The surgery did the work. A complete workup should not have to wait until someone is already in an IVF cycle. It should be the starting point.
However, moving forward with IVF is not a passive decision. Going in unprepared carries its own very real risk. A woman who goes into stimulation with unaddressed thyroid dysfunction, poor sleep, high cortisol, or nutritional gaps may not respond the way her baseline numbers suggested she would. Sperm quality on retrieval day is determined by what happened in the 70 to 90 days before.
Whole-body preparation before IVF is not optional wellness advice. It is risk reduction.
One more thing worth saying clearly: delaying IVF when it is the right choice also has a cost. IVF success rates decline with every year of age, and that decline accelerates after 35. Waiting out of fear, or because it does not feel natural, without actively working on your health in the meantime, can quietly cost you options. The goal is not to wait. The goal is to prepare intentionally and move forward informed.
What Actually Moves The Needle?
Both natural conception and IVF success come down to the same underlying biology and a lot of it is modifiable.
Egg quality matters enormously. Sperm health matters just as much and gets overlooked far too often. Male factor issues contribute to 40 to 50% of infertility cases and responds meaningfully to lifestyle changes in just 70 to 90 days. So does the uterine environment, shaped by inflammation, thyroid function, and metabolic health. A healthy embryo still needs the right environment to implant and grow. So do toxin exposure, oxidative stress, and nutrient status, all of which influence how eggs and sperm develop in the months before a cycle begins.
None of these are fully in a clinic's control. All of them are addressable and lead to better retrieval outcomes, better fertilization rates, and better implantation success than the same woman without that foundation. The same is true for natural conception.
IVF stimulates what is already there. Your job and ours is to make sure what is already there is as healthy as possible.
This Is Not About Rejecting IVF
And it is not about blindly jumping into it either.
It is about making a decision from a grounded, informed place, not from fear, pressure, or black and white thinking.
Whether you are optimizing naturally, preparing for IVF, or somewhere in between, you deserve a strategy that accounts for your whole body and your partner's health, not just the next procedure.
At WOVA we support you either way. You work with a coordinated team of experienced professionals who look at the full picture, not just the next step.
Because two healthy bodies give any path its best possible chance.
Work with WOVA → START HERE
P.S. Not sure if you’re ready to enroll? Take our free Fertility Quiz and find out what's actually missing from your picture.
References:
Wesselink AK, Rothman KJ, Hatch EE, Mikkelsen EM, Sørensen HT, Wise LA. Age and fecundability in a North American preconception cohort study. Am J Obstet Gynecol. 2017;217(6):667.e1-667.e8. doi:10.1016/j.ajog.2017.08.018
Centers for Disease Control and Prevention. 2022 Assisted Reproductive Technology National Summary Report. US Department of Health and Human Services; 2024.
Shingshetty L, Cameron NJ, Mclernon DJ, Bhattacharya S. Predictors of success after in vitro fertilization. Fertil Steril. 2024;121(5):742-751. doi:10.1016/j.fertnstert.2024.03.003
Rotimi DE, Singh SK. Implications of lifestyle factors on male reproductive health. JBRA Assist Reprod. 2024;28(2):320-330. doi:10.5935/1518-0557.20240007